Occupational Toxicity and How Toxicokinetic Function Shapes Risk, Monitoring, and Prevention
Abstract
Occupational toxicity remains a central concern in contemporary worker health because the severity of harm is determined not only by the hazardous properties of a substance but also by the way exposure is taken up, distributed, biotransformed, stored, and eliminated in the body. This article examines occupational toxicity through the lens of toxicokinetics, arguing that an adequate understanding of workplace risk requires movement beyond a simple inventory of hazardous agents toward an analysis of internal dose, target-organ delivery, and biological monitoring. Drawing on the literature in occupational and regulatory toxicology, the discussion outlines the core toxicokinetic processes of absorption, distribution, metabolism, and excretion, and shows how these processes mediate the relationship between external exposure and disease. Particular attention is given to benzene and lead, two classic occupational hazards whose differing toxicokinetic profiles illustrate why air monitoring alone is often insufficient. While benzene toxicity is strongly shaped by metabolic activation and hematopoietic susceptibility, lead presents a contrasting pattern characterised by prolonged storage in bone and chronic remobilisation into blood. The article further considers the implications of toxicokinetic knowledge for surveillance, biomarker selection, control hierarchies, and precautionary regulation. It concludes that occupational health practice is most defensible when toxicokinetic reasoning is integrated with industrial hygiene, clinical surveillance, and critical attention to worker variability.
Introduction
Occupational toxicity concerns the adverse effects produced when workers encounter chemical, biological, or mixed hazards in the course of employment. In its broadest sense, occupational toxicology applies the principles of toxicology to hazards arising in work environments, especially those encountered through inhalation, dermal absorption, and, less visibly but still importantly, ingestion through contaminated hands, food, or surfaces (Gupta, 2020). Yet the field is not reducible to hazard identification alone. A workplace chemical may be intrinsically dangerous and still present different levels of risk depending on concentration, route of entry, duration of exposure, co-exposures, and the physiological state of the exposed worker.
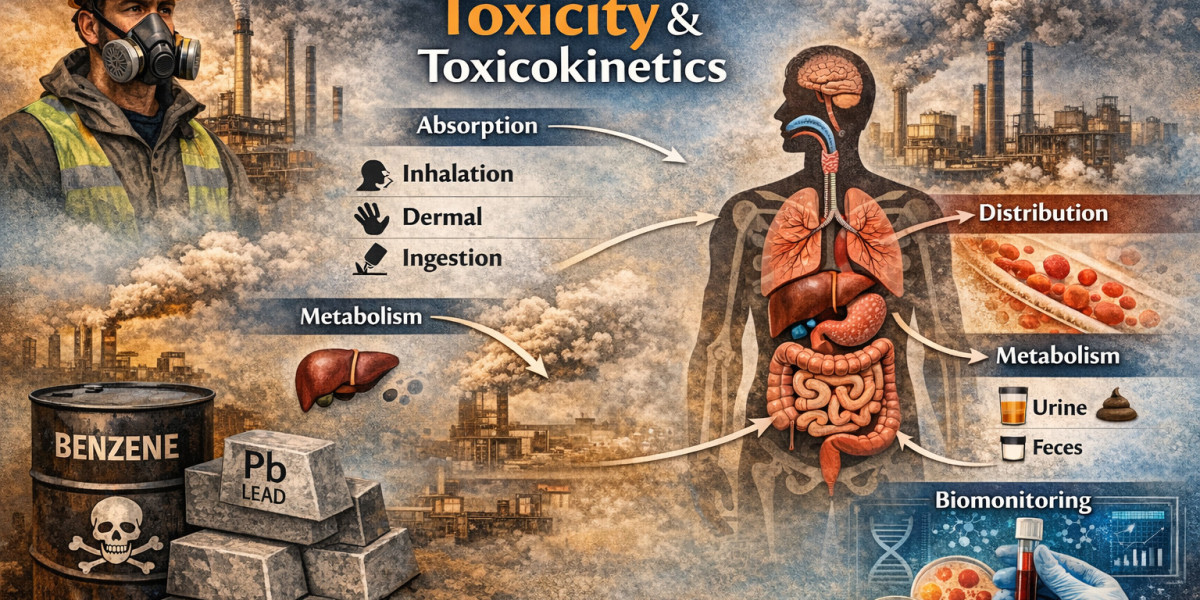
What complicates the matter further is that occupational disease rarely follows a straightforward line from external exposure to clinical outcome. Between the air concentration measured by an industrial hygienist and the pathology diagnosed by a physician lies a sequence of biological processes that determine internal dose. Those processes, conventionally grouped under toxicokinetics, are often described as absorption, distribution, metabolism, and excretion. The National Research Council has noted that toxicokinetic analysis is useful precisely because each of these processes may have its own dose and time dependence, making exposure assessment inseparable from temporal and physiological context (National Research Council, 2000).
This article argues that toxicokinetics is not a technical add-on to occupational toxicity but one of its organising logics. Put differently, toxicokinetic reasoning helps explain why two workers exposed to apparently similar concentrations may not experience comparable internal burdens or health outcomes. It also clarifies why surveillance programs, biological exposure indices, and control measures should not be designed solely around environmental measurements. In current scholarly debates, this is a recurring tension: some approaches privilege external exposure metrics, whereas others insist that internal dose and susceptibility are the more analytically meaningful anchors for prevention. The latter view, while not always simple to operationalise, is increasingly persuasive.
Occupational Toxicity as a Workplace Health Problem
The contemporary workplace contains a wide array of toxic agents, including solvents, metals, combustion products, pesticides, welding fumes, isocyanates, and process-generated contaminants. The NIOSH Pocket Guide to Chemical Hazards remains a widely used reference because it consolidates occupational exposure limits, physical properties, measurement methods, and protective recommendations for hundreds of agents encountered at work (NIOSH, 2024). Such tools are indispensable, but they can encourage an overly static view of toxicity if they are read merely as lists of hazards rather than as entry points into dynamic exposure pathways.
A stronger account of occupational toxicity situates toxic substances within labour processes and material conditions. Workers in petrochemical operations, battery manufacture and recycling, painting, printing, e-waste processing, laboratory settings, mining, and informal industrial sectors may confront repeated low-dose exposure rather than dramatic poisoning episodes. That distinction matters. Acute toxicity has historically shaped regulation because it is visible and often catastrophic. Chronic occupational toxicity, by contrast, may emerge gradually through cumulative dose, latency, and biologically retained burden. In this respect, the field has long wrestled with a difficult question: should prevention focus primarily on threshold-based compliance, or should it be guided by the possibility that some toxic effects occur at levels once assumed to be acceptable? The benzene literature, for example, has repeatedly unsettled confidence in sharp thresholds for hematotoxic effects (Smith, 2010).
Another point worth emphasising is that occupational toxicity is socially distributed. Work organisation, subcontracting, inadequate ventilation, inconsistent use of personal protective equipment, and weak surveillance infrastructures often shape who bears the highest burden. Therefore, a toxicological analysis that ignores power, enforcement, and access to protection risks becoming descriptively thin. The chemistry of a toxicant matters, but so does the political economy of exposure.
How Toxicokinetic Function Operates
Toxicokinetics concerns what the body does to a xenobiotic over time. In analytical terms, it addresses uptake, movement between compartments, biotransformation, storage, and elimination. The National Research Council separates these processes into absorption and elimination, with biotransformation, distribution, and excretion treated as overlapping but distinct determinants of internal dose (National Research Council, 2000). Although this formulation is familiar, its practical significance in occupational health deserves careful restatement.
Absorption is the point at which the workplace environment becomes biologically consequential. In occupational settings, inhalation is often the dominant route because many hazards are present as vapours, aerosols, gases, dusts, or fumes. Dermal uptake, however, may be underestimated, especially with liquid solvents, pesticides, and compounds capable of crossing the skin barrier. Oral intake is sometimes treated as secondary, yet hand-to-mouth transfer remains an important pathway where hygiene is poor. The critical issue is not merely whether a substance is present in the workplace, but whether, how quickly, and by which route it enters systemic circulation.
Once absorbed, a toxicant is distributed through blood and tissues. Distribution is shaped by perfusion, tissue affinity, lipid solubility, protein binding, and, in some cases, sequestration in specific organs. At this stage, toxicology begins to diverge from simplistic exposure thinking. The target organ is not always the first site of entry. Nor is blood concentration always a stable surrogate for total body burden. Distribution may create hidden reservoirs that make a worker appear less exposed than the longer biological story would suggest.
Metabolism, often occurring in the liver but not exclusively there, can either detoxify or bioactivate a compound. This is where toxicokinetics intersects most sharply with mechanism. It is sometimes assumed in lay discussion that metabolism makes chemicals safer by preparing them for excretion. That is only partly true. For several occupational toxicants, the metabolite is more damaging than the parent compound. Biotransformation therefore mediates toxicity in ways that are both chemically specific and biologically variable, depending on enzyme activity, genetic polymorphism, co-exposure, smoking status, nutrition, and disease state.
Excretion, finally, removes the parent compound or its metabolites through urine, bile, faeces, sweat, exhaled air, or other routes. Yet elimination should not be confused with prompt clearance. A toxicant with prolonged storage or slow release may continue to exert effects long after active exposure has declined. From an occupational health standpoint, that temporal lag is crucial because it complicates return-to-work decisions, interpretation of biomarkers, and confidence in exposure reduction programs.
Benzene as a Toxicokinetic Case Study
Benzene remains one of the clearest illustrations of why occupational toxicity must be understood through toxicokinetic function. OSHA continues to regulate benzene tightly, requiring exposure monitoring, medical surveillance, and removal protections under specified conditions (OSHA, n.d.-a). This regulatory architecture reflects a long history of evidence linking benzene to bone marrow toxicity and haematological malignancy.
From a toxicokinetic perspective, benzene is primarily an inhalation hazard, though dermal absorption can also occur with liquid contact (OSHA, n.d.-b). The deeper issue, however, lies in metabolism. Benzene itself is not the whole toxicological story. Its metabolites, generated through enzymatic oxidation and further transformation, are central to the damage observed in hematopoietic tissues. ATSDR's toxicological profile and subsequent reviews describe benzene metabolism as quantitatively important because species differences and tissue-specific activation affect the formation of toxic intermediates in bone marrow and related compartments (Agency for Toxic Substances and Disease Registry [ATSDR], 2007; Smith, 2010).
This has important implications for exposure assessment. Air benzene concentration is clearly relevant, but it does not by itself capture internal dose or the efficiency with which the compound is converted into harmful metabolites. Rahimpoor et al. (2023), in a systematic review of biological exposure indices, concluded that biomarker choice should vary with exposure level and that smoking, diet, and genetic polymorphism can confound interpretation. At low concentrations, unmetabolised benzene in urine or exhaled air may be more informative; at moderate concentrations, urinary trans,trans-muconic acid and S-phenylmercapturic acid may be more useful. The significance of this literature is methodological as much as clinical: toxicokinetics explains why biomonitoring cannot be treated as a one-size-fits-all exercise.
The benzene debate also exposes an unresolved regulatory tension. Some occupational standards remain rooted in threshold assumptions and compliance logic, whereas parts of the scientific literature suggest that hematotoxic effects may occur at very low concentrations and perhaps without a clear safe threshold (Smith, 2010). One need not resolve that debate absolutistically to appreciate its consequence. Where uncertainty persists, a precautionary reading of toxicokinetic and epidemiologic evidence is often more defensible than a narrow reliance on nominal compliance.
Lead as a Toxicokinetic Case Study
Lead presents a markedly different toxicokinetic pattern and therefore a different occupational challenge. Inorganic lead exposure remains important in battery manufacture, recycling, smelting, construction, firing ranges, and related industries. OSHA's lead standard has long relied on biological monitoring, especially blood lead and zinc protoporphyrin testing, to guide surveillance and medical management (OSHA, n.d.-c). More recent CDC guidance similarly emphasises blood lead surveillance and recommends increasingly protective responses at lower blood lead concentrations than older regulatory practice often assumed (CDC, 2024).
The reason blood monitoring matters becomes clearer when one considers distribution and storage. According to ATSDR, in adults roughly 94% of total lead body burden is stored in bone, where it can remain for prolonged periods and later re-enter circulation (ATSDR, 2020). This is a classic example of toxicokinetics altering the meaning of current exposure data. A worker's blood lead concentration may reflect not only recent uptake but also mobilisation from skeletal stores. Consequently, exposure reduction does not always translate into immediate biological normalisation.
Lead toxicokinetics therefore complicates both diagnosis and prevention. External air sampling remains necessary, especially for compliance and source control, but it is not sufficient. Bone storage, redistribution, and variable elimination mean that cumulative burden may matter more than a single environmental snapshot. The National Research Council's earlier work on biologic monitoring made this point in a broader sense, arguing that interpretation of biomarkers depends on a toxicokinetic and physiological framework rather than on screening data alone (National Research Council, 1993). In practical terms, this is why occupational lead programs that rely only on area measurements risk missing the longer biological consequences of repeated exposure.
There is also a policy implication here. Although OSHA standards retain historically important triggers, newer occupational health recommendations are often more conservative. CDC summarises guidance from ACOEM, CDPH, and related bodies suggesting medical removal or more frequent follow-up at blood lead levels well below older regulatory thresholds (CDC, 2024). This divergence between regulatory minima and health-protective recommendations is not merely bureaucratic. It reflects a growing recognition that toxicokinetic persistence and subclinical effects challenge the adequacy of older assumptions.
Why Toxicokinetics Matters for Occupational Health Practice
If toxicokinetics is taken seriously, several practical consequences follow. First, monitoring strategies should combine environmental and biological data wherever feasible. The selection of biomarkers must be substance-specific and sensitive to exposure scenario, timing of sample collection, and confounding variables. Second, medical surveillance should not be limited to detecting manifest disease. Its purpose is also anticipatory: to identify internal dose patterns and early biological effects before irreversible injury develops. OSHA's benzene standard, for instance, requires medical surveillance for defined categories of exposed workers, thereby recognising that prevention cannot rely on symptoms alone (OSHA, n.d.-a).
Third, toxicokinetic knowledge should sharpen the hierarchy of controls rather than displace it. There is a risk, especially in highly monitored industries, that biomonitoring can become a substitute for engineering control. That would be a mistake. Biomarkers tell us that uptake has occurred; they do not prevent it. The more defensible model is one in which toxicokinetics informs control design by clarifying route, retention, and target-organ relevance, while elimination, substitution, enclosure, ventilation, work practice controls, and appropriate personal protective equipment remain the primary means of reducing harm.
Fourth, toxicokinetics encourages attention to worker variability. Smoking, alcohol use, nutritional status, age, pregnancy, renal function, prior body burden, genetic polymorphisms, and co-exposure profiles may alter internal dose and effect. This does not justify shifting responsibility from employers to workers. Rather, it should remind practitioners that a uniform exposure limit may not protect all members of a workforce equally. In that respect, occupational toxicology increasingly overlaps with debates about vulnerability, equity, and the ethics of standard setting.
Conclusion
Occupational toxicity is best understood not as a simple property of hazardous substances but as a dynamic relation between workplace exposure and the body's handling of that exposure. Toxicokinetic function provides the bridge between external concentration and biological effect. By tracing how toxicants are absorbed, distributed, metabolised, stored, and excreted, it becomes possible to explain why disease patterns differ across agents, tasks, and workers, and why environmental compliance alone may fail to capture true risk.
Benzene and lead make this argument in different ways. Benzene shows how metabolic activation and hematopoietic targeting can make even apparently low exposures consequential. Lead demonstrates how storage in bone and slow remobilisation turn exposure into a long temporal problem rather than a momentary event. In both cases, toxicokinetics complicates complacent readings of workplace data and supports a more integrated model of prevention.
For occupational health professionals, the implication is clear enough. Hazard recognition must be linked to toxicokinetic understanding, biomonitoring must be interpreted cautiously and contextually, and regulatory compliance should be treated as a floor rather than an endpoint. A mature occupational toxicology practice is therefore not only scientific. It is also interpretive, preventive, and ethically attentive to the workers whose bodies carry the burden of industrial production.
References
Agency for Toxic Substances and Disease Registry. (2007). Toxicological profile for benzene. U.S. Department of Health and Human Services. https://www.atsdr.cdc.gov/toxprofiles/tp3.pdf
Agency for Toxic Substances and Disease Registry. (2020). Toxicological profile for lead. U.S. Department of Health and Human Services. https://www.atsdr.cdc.gov/toxprofiles/tp13.pdf
Centers for Disease Control and Prevention. (2024, April 11). Blood lead level guidance. National Institute for Occupational Safety and Health. https://www.cdc.gov/niosh/lead/bll-reference/index.html
Gupta, P. K. (2020). Occupational toxicology. In D. M. Roberts, J. Buckley, & S. L. Greene (Eds.), The concise guide to pharmacology and toxicology for clinical and forensic scientists (pp. 559-577). Springer. https://doi.org/10.1007/978-3-030-50409-0_24
National Institute for Occupational Safety and Health. (2024). NIOSH pocket guide to chemical hazards. Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/npg/default.html
National Research Council. (1993). Biologic markers of lead toxicity. National Academies Press. https://www.ncbi.nlm.nih.gov/books/NBK236462/
National Research Council. (2000). Approaches for using toxicokinetic information in assessing risk to deployed U.S. forces. In Strategies to protect the health of deployed U.S. forces: Assessing health risk of deployed U.S. forces (pp. 56-80). National Academies Press. https://www.ncbi.nlm.nih.gov/books/NBK225064/
Occupational Safety and Health Administration. (n.d.-a). 1910.1028 - Benzene. U.S. Department of Labor. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1028
Occupational Safety and Health Administration. (n.d.-b). Medical surveillance guidelines for benzene. U.S. Department of Labor. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1028AppC
Occupational Safety and Health Administration. (n.d.-c). 1910.1025 App B - Employee standard summary. U.S. Department of Labor. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1025AppB
Rahimpoor, R., Kaveh, M., Fakhrinnia, M., Omidi, L., Soleimani, E., & Ghamari, F. (2023). Biological exposure indices of occupational exposure to benzene: A systematic review. Heliyon, 9(11), e21549. https://doi.org/10.1016/j.heliyon.2023.e21549
Smith, M. T. (2010). Advances in understanding benzene health effects and susceptibility. Annual Review of Public Health, 31, 133-148. https://doi.org/10.1146/annurev.publhealth.012809.103646
Professional Review Article
Author: Wilson Ronnie Odoom, ASHEPA President
Engr., QHSE, NEBOSH, FASHEPA






